Carpal tunnel syndrome is a common condition in which the median nerve is compressed as it passes through the carpal tunnel at the wrist. It causes numbness, tingling, and weakness in the thumb, index, middle, and half of the ring finger. Symptoms often wake patients at night and worsen with gripping, typing, or driving. Treatment ranges from night splinting and corticosteroid injection to endoscopic surgical release, which Dr. Loredo performs through a micro incision with no stitches and recovery measured in days.
The Anatomy of the Carpal Tunnel
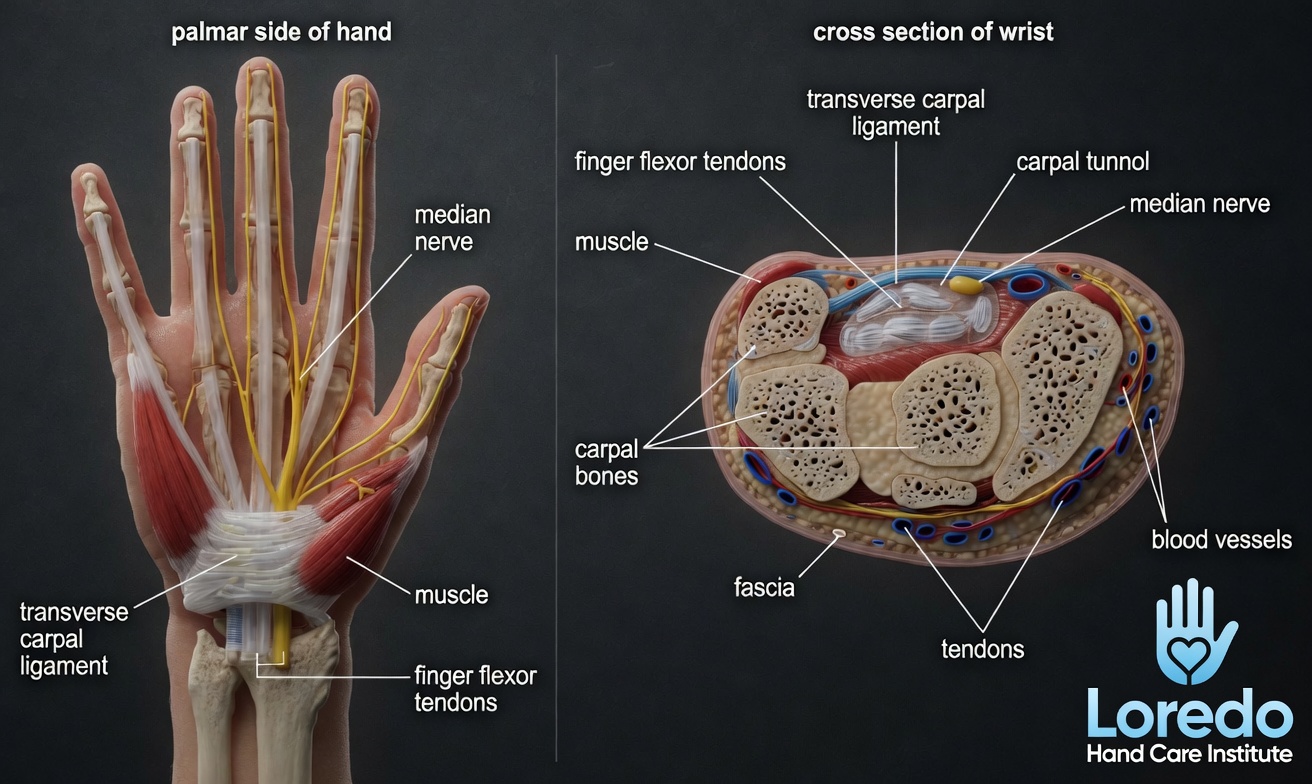
The carpal tunnel is a narrow fibrous-osseous passage at the base of the palm. The bones of the wrist form three sides and the transverse carpal ligament forms the roof. Nine flexor tendons and the median nerve pass through this tunnel to reach the hand. The median nerve controls sensation to the thumb, index finger, middle finger, and the thumb-side half of the ring finger. It also powers the small thenar muscles at the base of the thumb, which is why advanced cases can present with thumb weakness and visible muscle thinning.
Clinical coding: ICD-10 G56.0 (carpal tunnel syndrome). SNOMED CT 57406009.
Causes and Risk Factors
Carpal tunnel syndrome develops when the pressure inside the carpal tunnel rises or the tunnel itself narrows. Common contributors:
- Repetitive forceful gripping (construction, manual trades, manufacturing)
- Prolonged wrist-flexed postures (keyboard use with poor ergonomics, sustained phone holding)
- Pregnancy, especially the third trimester (usually resolves after delivery, but not always)
- Diabetes, hypothyroidism, rheumatoid arthritis, and other systemic conditions
- Prior wrist fracture or dislocation that altered the shape of the tunnel
- Age (most common between 40 and 60)
Women are affected two to three times more often than men. The condition is bilateral in roughly half of patients.
Symptoms and Warning Signs
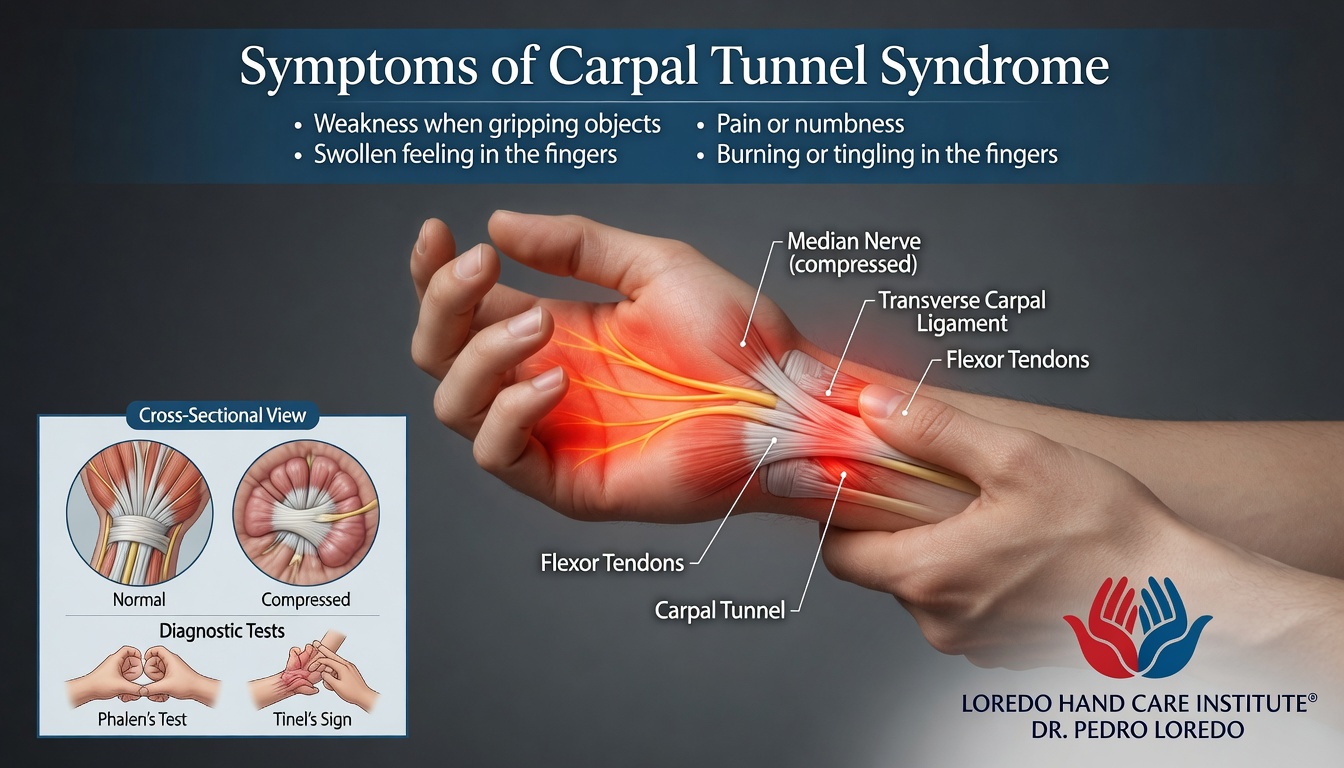
- Numbness or tingling in the thumb, index, middle, and half of the ring finger
- Symptoms that wake you at night or appear first thing in the morning
- Shaking the hand to relieve symptoms (the flick sign)
- Weakness of grip and difficulty with fine pinch tasks
- Dropping objects or losing track of items held in the hand
- Trouble with fine tasks like buttoning shirts, picking up coins, or turning a key
- In advanced cases, visible thinning of the thenar muscles at the base of the thumb
How the Diagnosis Is Made
The diagnosis begins with a focused history and a hand examination. Dr. Loredo performs standard provocative tests:
- Tinel sign at the wrist: tapping over the median nerve at the wrist reproduces tingling in the median-nerve distribution.
- Phalen maneuver: holding the wrists fully flexed for 60 seconds reproduces numbness or tingling.
- Durkan carpal compression test: direct pressure on the median nerve at the wrist for 30 seconds reproduces symptoms. This is the most sensitive bedside test.
When the diagnosis is uncertain or surgery is contemplated, electrodiagnostic studies (EMG and nerve conduction studies) confirm the location and grade the severity. Ultrasound imaging of the median nerve is available when clinically indicated and can show the nerve swelling or flattening as it enters the tunnel.
Non-Surgical Treatment Options
- Night wrist splinting in a neutral position. Splinting during sleep prevents the wrist-flexed postures that spike pressure in the tunnel. Often resolves mild cases entirely when used consistently.
- Activity modification and ergonomic correction. Adjusting keyboard height, wrist posture, and grip technique at work and home.
- Oral medications. Non-steroidal anti-inflammatory medications (NSAIDs) such as ibuprofen or naproxen reduce inflammation around the median nerve and ease pain. Acetaminophen helps with pain relief. In select cases, a short course of oral corticosteroids or a gabapentinoid for nerve pain is appropriate. Dr. Loredo reviews medical history, current medications, and contraindications before recommending any prescription option.
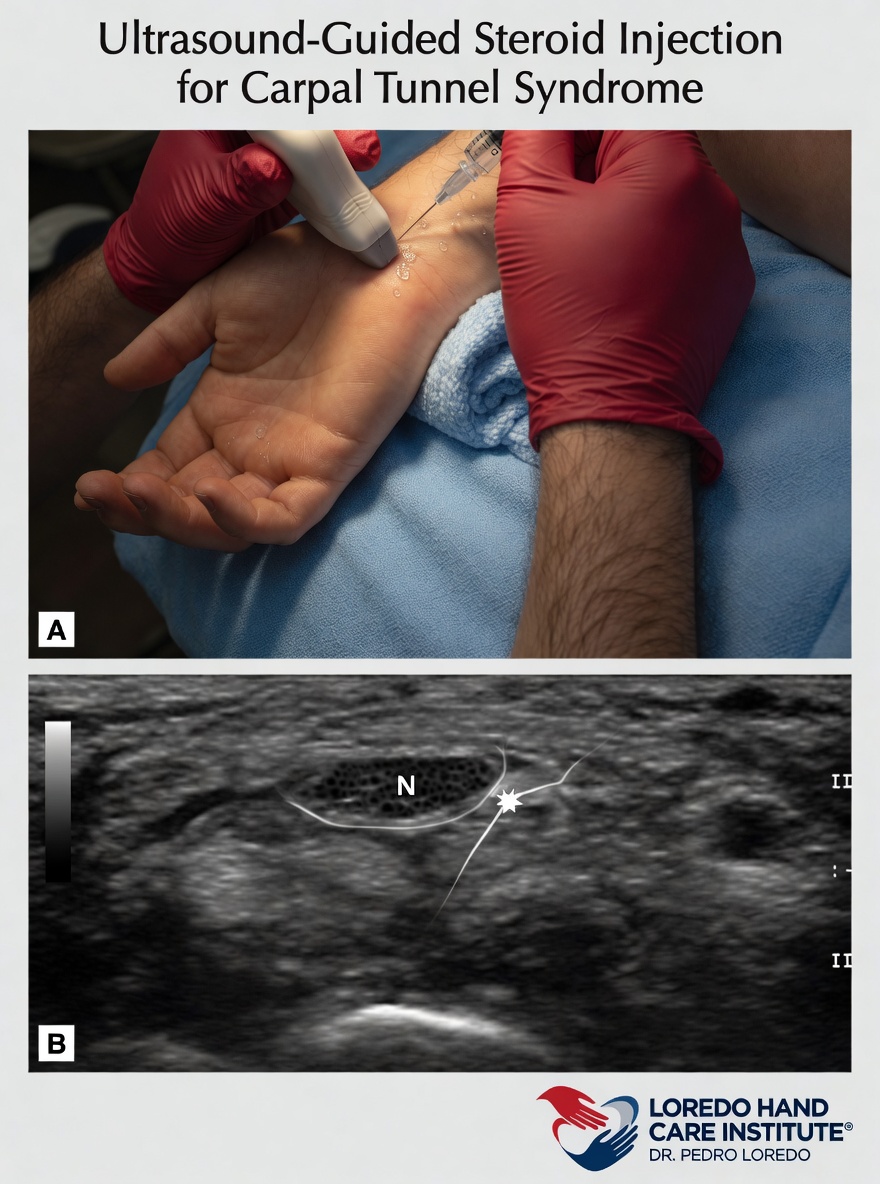
- Corticosteroid injection into the carpal tunnel. Reduces nerve inflammation and relieves symptoms in many patients. Injections are repeatable, but if symptoms return quickly or a second injection fails, surgical release becomes the definitive option.
- Targeted hand therapy with a certified hand therapist, including nerve and tendon gliding exercises.

Surgical Options
Surgical release divides the transverse carpal ligament, immediately reducing pressure on the median nerve. Two approaches:
Endoscopic Carpal Tunnel Release (Dr. Loredo's preferred approach)
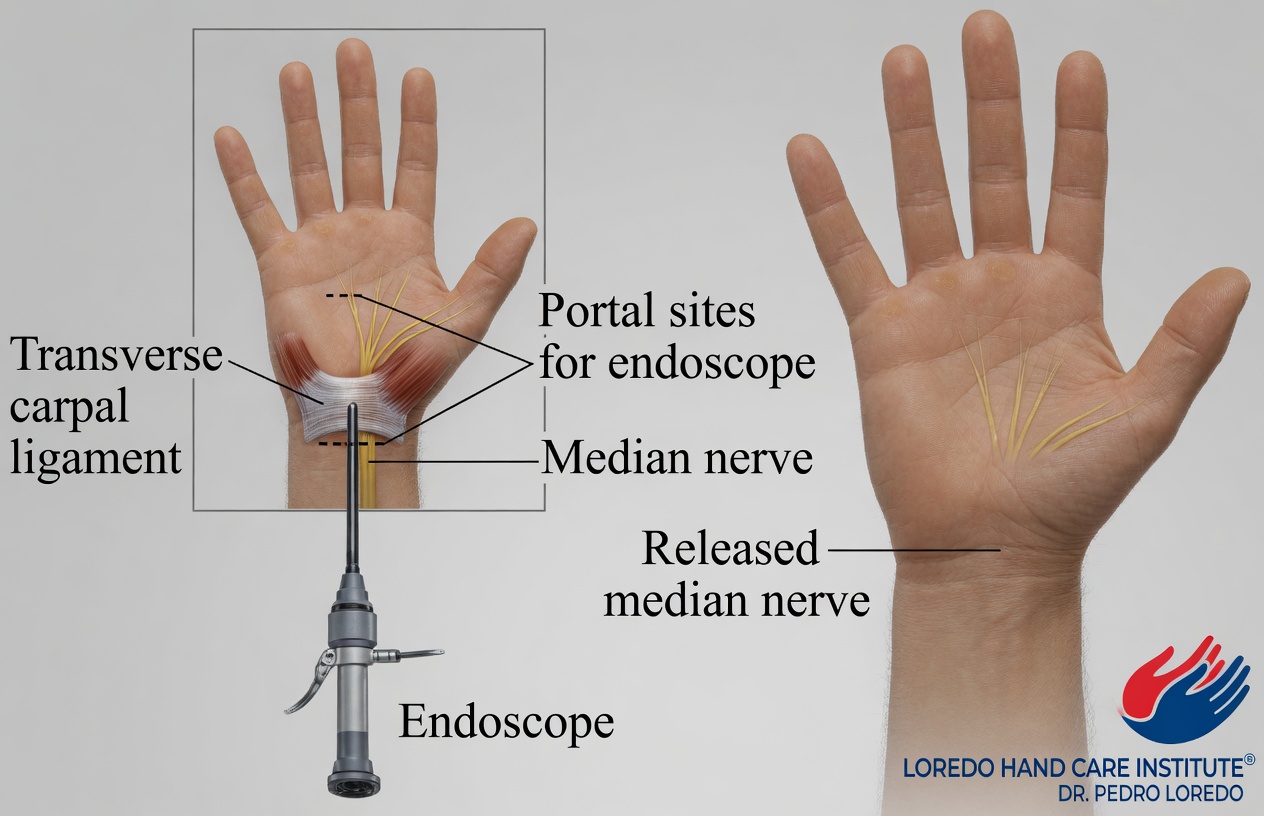
- Advanced minimally invasive technique
- Single micro incision at the wrist, smaller than a grain of rice
- Complete division of the transverse carpal ligament under direct visualization
- No skin sutures
- Preserves the palmar fat pad that open release disrupts
- Reduced scar tenderness and palmar pillar pain
- Most patients return to light function the same day
For the full procedure walk-through, see Endoscopic Carpal Tunnel Release.
Open Carpal Tunnel Release
- Traditional approach with a longer palm incision
- Appropriate for revision surgery, certain anatomic variations, or patient preference
- Requires skin sutures that are removed at the two-week visit
- Recovery is slightly longer than endoscopic, with more pillar pain in the first weeks
Dr. Loredo reviews both options in detail at your consultation and recommends the approach best suited to your anatomy, severity, and lifestyle.
Recovery Timeline
- Day 0: Procedure performed in about 10 to 15 minutes under local anesthesia with light sedation. Gentle finger motion begins the same day.
- Day 1 to 3: Light hand use for routine daily activity. Bandage care per discharge instructions.
- Week 1 to 2: Most patients return to desk work. First follow-up visit. Any sutures removed (endoscopic release typically has none).
- Week 2 to 4: Grip strength exercises, tendon and nerve gliding. Pillar pain may be present and is expected.
- Week 4 to 6: Return to heavier activity, including manual labor and athletics, as tolerated.
- Month 2 to 6: Full grip strength continues to improve. Nerve recovery progresses over months in severe cases. Scar softens and flattens.
Returning to Work and Daily Activity
Return-to-work timing depends on the type of work and the surgical approach used.
- Office or desk work: 2 to 7 days after endoscopic release. 7 to 14 days after open release.
- Manual labor or heavy gripping: 4 to 6 weeks, typically with a gradual return through light duty first.
- Driving: 1 to 7 days after endoscopic release, once you are off narcotic pain medication and can grip the steering wheel confidently. 1 to 2 weeks after open release.
- Exercise and sports: light cardio and lower-body exercise in week 1. Upper-body resistance training after week 4.
Frequently Asked Questions
How long is recovery from carpal tunnel surgery?
With endoscopic release through a micro incision, most patients use the hand lightly the same day, return to desk work within 2 to 7 days, and resume heavier activity within 4 to 6 weeks. Nerve recovery continues over months in severe cases. Recovery varies by individual and by how severe the nerve compression was before surgery.
Will my numbness fully go away after carpal tunnel surgery?
Mild to moderate cases typically see numbness improve over weeks. Severe, long-standing nerve compression can take 6 to 12 months or longer for full nerve recovery, and in the most advanced cases some residual numbness may remain. Earlier treatment leads to more complete recovery.
Is carpal tunnel surgery painful?
The procedure is performed with local anesthesia and light sedation. Post-operative soreness is typically mild and most patients manage with over-the-counter acetaminophen or ibuprofen. Narcotic medication is rarely needed beyond the first day.
When can I drive after carpal tunnel surgery?
After endoscopic carpal tunnel release, most patients drive again within 1 to 7 days, once they are off narcotic pain medication and can grip the steering wheel without discomfort. After open release, driving typically resumes around 1 to 2 weeks.
What if my carpal tunnel symptoms come back after surgery?
Recurrence after complete release is uncommon. When symptoms persist, the most likely causes are incomplete prior release, scar tissue, or a second site of nerve compression elsewhere in the arm. A fellowship-trained hand surgeon can evaluate the specific pattern and recommend next steps.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Numbness or tingling that wakes you at night on multiple nights per week
- Dropping objects or losing grip strength in routine tasks
- Symptoms that have not improved after 4 to 6 weeks of night splinting
- Visible thinning of the muscle at the base of the thumb
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage from the wound
- Severe pain that is not controlled by over-the-counter medication
- Numbness that worsens rather than improves
- Sudden new finger stiffness or inability to straighten the fingers
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow, which causes numbness in the ring and small fingers rather than the thumb side of the hand. Can coexist with carpal tunnel syndrome.
- Trigger Finger: a tendon problem, not a nerve problem, that often coexists with carpal tunnel, especially in diabetic patients.
- De Quervain's Tendonitis: thumb-side wrist pain from inflamed tendons. Sometimes confused with carpal tunnel because of thumb involvement.
- Thumb Basilar Joint Arthritis: thumb-base pain from joint wear. Different mechanism, but thumb weakness from CTS and CMC arthritis can look similar.
- Endoscopic Carpal Tunnel Release (procedure): full procedure detail including before, day-of, and recovery expectations.
From the Blog
- Early Signs of Carpal Tunnel: night numbness, dropping objects, weak pinch, and the flick sign.
- What to Expect After Carpal Tunnel Surgery: week-by-week recovery from endoscopic release.
- Night Splints for Carpal Tunnel: how splints work and how long to try them.
- How to Prevent Carpal Tunnel from Computer Work: ergonomics, breaks, and risk factors.
- The Median Nerve Explained: nerve anatomy and the four main compression sites.
Watch: Carpal tunnel educational videos
Short videos from Dr. Loredo's YouTube, Instagram, and Facebook channels.