Trigger finger (stenosing tenosynovitis) is a common condition in which a finger catches, clicks, or locks when you try to bend or straighten it. The problem occurs when the flexor tendon that bends the finger no longer glides smoothly through a tight pulley in the palm called the A1 pulley. The thumb, ring, and middle fingers are most often affected. Mild cases often respond to splinting and a single corticosteroid injection. Persistent locking is treated with a short outpatient release of the A1 pulley by Dr. Loredo, with patients typically using the hand the same day.
The Anatomy Behind Trigger Finger
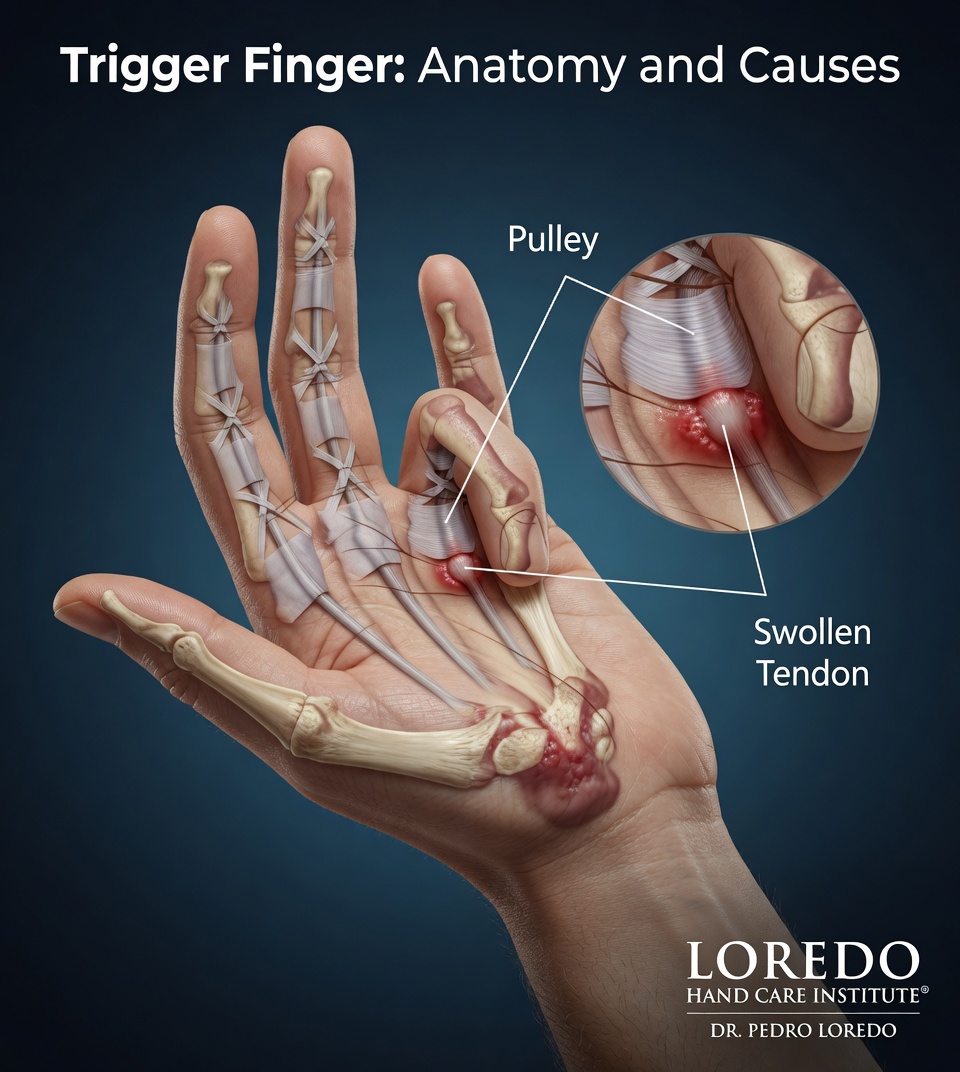
Each finger has two flexor tendons (the thumb has one) that travel from the forearm through a series of narrow tunnels in the palm and finger called pulleys. The A1 pulley is the first of these tunnels in the palm, located at the base of the finger where the finger meets the palm. In trigger finger, thickening of the tendon, the sheath around it, or both, causes the tendon to catch as it passes through the narrowed A1 pulley. You feel the catch as a click, snap, or lock.
Clinical coding: ICD-10 M65.3 (trigger finger). SNOMED CT 202790003 (stenosing tenosynovitis).
Causes and Risk Factors
Trigger finger can develop spontaneously or after a period of repetitive or forceful gripping. Known risk factors:
- Repetitive or sustained gripping (tools, steering wheels, sports equipment, gardening)
- Diabetes: significantly increases risk, is associated with multiple-finger involvement, and reduces the success rate of cortisone injection
- Rheumatoid arthritis
- Hypothyroidism
- Amyloidosis
- Age 40 to 60
- Female sex: three to six times more common in women
The thumb is the most commonly affected digit, followed by the ring and middle fingers. In diabetic patients, multiple fingers may be involved simultaneously.
Symptoms and Warning Signs
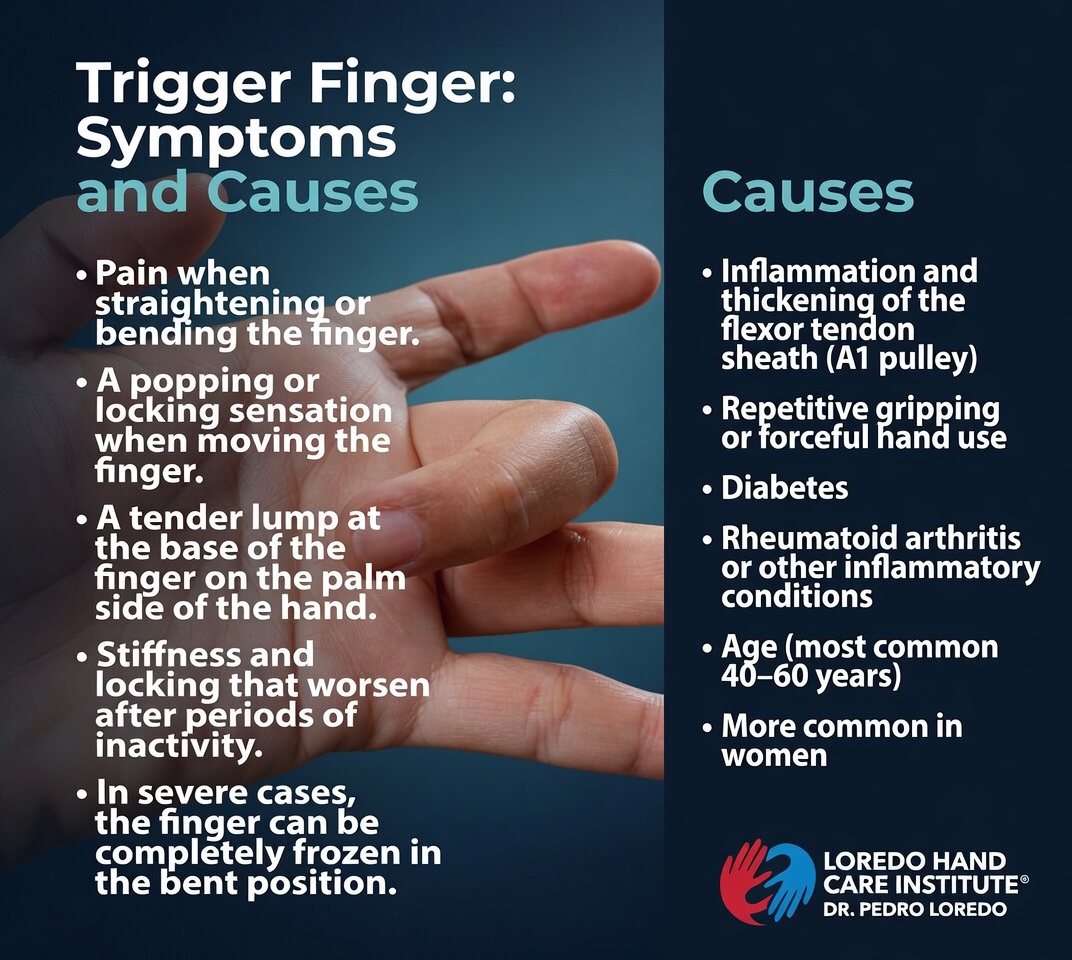
- A finger catches, clicks, or snaps when you bend or straighten it
- A tender, palpable nodule in the palm at the base of the affected finger
- Pain that worsens with gripping or in the morning after prolonged flexion during sleep
- A finger that locks in a bent position and must be pulled straight with the other hand
- Stiffness of the finger, especially on first waking
- In advanced cases, a finger that will not fully bend or straighten
- In late-stage disease, a fixed flexion contracture of the finger at the PIP joint
How the Diagnosis Is Made
Trigger finger is a clinical diagnosis. Imaging is rarely required. Dr. Loredo's examination includes:
- Palpation of the A1 pulley region, which often reveals a tender thickened nodule
- Active finger flexion and extension to reproduce the catching or locking
- Observation of any finger locked at rest
- Range of motion assessment to identify any fixed contracture that would affect treatment
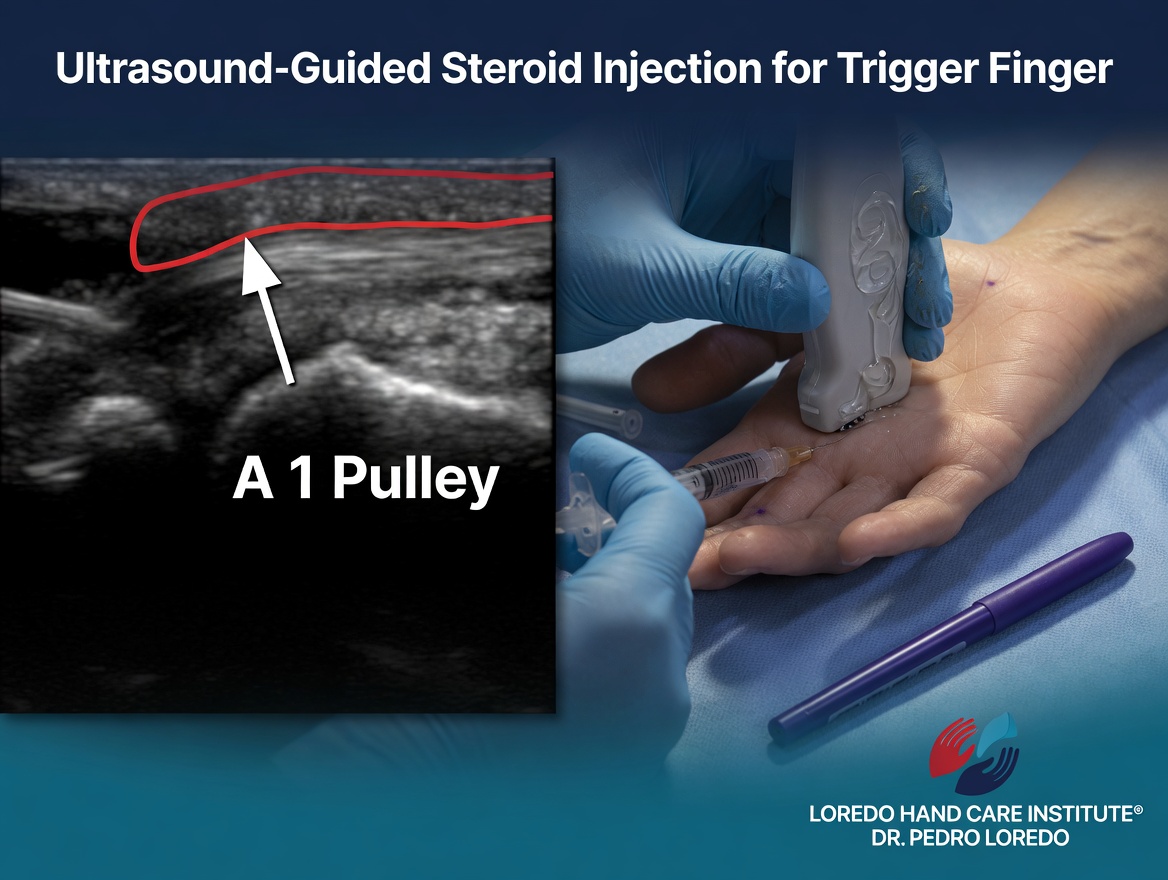
Ultrasound can visualize the thickened tendon or sheath when the clinical picture is atypical, but routine imaging is not needed for a straightforward diagnosis.
Non-Surgical Treatment Options
- Activity modification: reducing sustained gripping, heavy grip-and-release tasks, or prolonged impact to the affected finger.
- Night splinting: a small splint holds the finger straight at night and reduces morning catching in mild cases.
- Oral medications. Non-steroidal anti-inflammatory medications (NSAIDs) such as ibuprofen or naproxen reduce inflammation around the A1 pulley and ease pain. Acetaminophen helps with pain relief. Dr. Loredo reviews medical history, current medications, and contraindications before recommending any prescription option.
- Ultrasound-guided corticosteroid injection into the flexor tendon sheath at the A1 pulley. Success rate is roughly 60 percent in non-diabetic, first-time patients. Lower in diabetic patients. An injection is repeatable once; three or more injections in the same finger are not recommended because they raise the risk of tendon injury.
- Gentle tendon-gliding exercises to maintain smooth tendon excursion.


Surgical Options
When conservative care and corticosteroid injection fail to resolve the catching, surgical release of the A1 pulley is the definitive treatment. The procedure divides the A1 pulley under direct visualization, immediately eliminating the mechanical obstruction that causes the catching.
Open A1 Pulley Release (Dr. Loredo's surgical approach)

- Short outpatient procedure under local anesthesia, no general anesthesia required
- Small 1 to 2 cm incision at the distal palmar crease over the A1 pulley
- Direct visualization of the A1 pulley with full protection of the digital nerves and blood vessels
- Complete division of the A1 pulley under direct visualization, the most reliable way to ensure full release
- Identification and protection of any anatomic variations that a closed technique would risk missing
- Immediate resolution of the catching in nearly all patients
- Procedure time about 10 to 15 minutes
- Skin sutures placed and removed at the two-week follow-up visit
- Light hand use the same day, return to desk work within a few days
Open A1 pulley release has the longest track record, the highest reported success rate, and the lowest reported risk of incomplete release or digital nerve injury. Dr. Loredo performs every trigger finger surgery using the open approach to give every patient the safest, most reliable release.
Recovery Timeline
- Day 0: Procedure performed in about 10 to 15 minutes under local anesthesia. Light hand use the same evening.
- Day 1 to 3: Routine light daily activity. Catching and locking resolved immediately.
- Week 1: Most patients return to desk work. Bandage usually removed.
- Week 2 to 4: Return to heavier activity, including gripping and manual labor, as tolerated.
- Month 2: Full grip strength typically recovered.
- Month 3: Scar softening complete in most patients.
Returning to Work and Daily Activity
- Office or desk work: 2 to 5 days
- Manual labor or heavy gripping: 2 to 4 weeks. Start with light duty if the job requires heavy tool use.
- Driving: 1 to 3 days, once the hand grip feels secure and you are off narcotic pain medication
- Exercise and sports: light cardio immediately. Resume gripping or racket sports after week 2 to 4 based on comfort.
Frequently Asked Questions
Is a cortisone shot enough to fix trigger finger?
A single corticosteroid injection resolves trigger finger in roughly 60 percent of first-time, non-diabetic cases. Diabetic patients respond less predictably. When symptoms return after one or two injections, surgical release is the definitive treatment and has a very high success rate.
How fast is recovery from trigger finger surgery?
The procedure takes about 10 to 15 minutes under local anesthesia. Most patients use the hand lightly the same day, return to desk work within a few days, and resume heavier activity within two to four weeks.
Can more than one trigger finger be treated at once?
Yes. Multiple trigger digits are commonly released in a single visit when clinically appropriate. This saves the patient from multiple recovery periods and is well tolerated.
What if the catching returns after surgery?
Recurrence after complete A1 pulley release is uncommon. If catching returns, the cause is typically scar tissue or an incompletely divided pulley. A second-look evaluation by a fellowship-trained hand surgeon can identify the issue and recommend next steps.
Can diabetes make trigger finger harder to treat?
Yes. Diabetic patients are more likely to develop trigger finger, more likely to have multiple fingers affected, and less likely to respond fully to corticosteroid injection. Surgical release in diabetic patients has similar success to non-diabetic patients and is often the right first step when multiple fingers are involved.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- A finger that locks in a bent position and has to be pulled straight
- Catching that has not improved after 2 to 4 weeks of activity modification or splinting
- A tender, palpable nodule in the palm at the base of a finger
- More than one finger involved, especially if you have diabetes
- New catching along with a loss of full finger motion
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage from the wound
- Severe pain that is not controlled by over-the-counter medication
- Sudden loss of finger motion or inability to straighten the finger
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Carpal Tunnel Syndrome: a different mechanism (nerve compression, not a tendon problem), but often coexists with trigger finger, especially in diabetic patients.
- De Quervain's Tendonitis: a tendon problem in a different compartment (first dorsal compartment of the wrist, not the A1 pulley). Thumb-side wrist pain rather than finger catching.
- Thumb Basilar Joint Arthritis: joint wear at the base of the thumb. Thumb pain and weakness; different from trigger thumb, which is a tendon problem.
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow. A separate diagnosis but worth screening when a patient presents with grip weakness.
- Open A1 Pulley Release: surgical release of the A1 pulley when conservative care and corticosteroid injection have failed. Performed in office under local anesthesia in about 10 to 15 minutes. Detailed above in the Surgical Options section.
From the Blog
- Trigger Finger: Signs You Need to See a Hand Surgeon: five red flags warranting evaluation.
- When to See a Hand Surgeon for Trigger Finger: catching versus locking and the cortisone lifecycle.
- Trigger Finger Release Recovery: same-day full motion and the shortest recovery in hand surgery.
- Home Exercises for Trigger Finger: tendon glide sequence and what NOT to do.
- When a Cortisone Injection Is the Right Choice: trigger finger is the gold-standard injection candidate.
Watch: Trigger finger educational videos
Short videos from Dr. Loredo's YouTube, Instagram, and Facebook channels.